The eye behaves like a camera with the lens focusing light onto the retina rather than the film or image sensor. The retina converts light into impulses that travel up the optic nerve to the brain.
Anatomy of the Eye
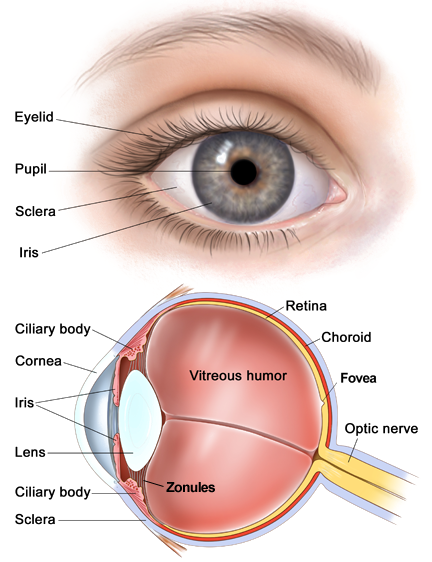
Cornea
The cornea is the transparent, dome-shaped window covering the front of the eye. It is a powerful refracting surface, providing 2/3 of the eye’s focusing power. Like the crystal on a watch, it gives us a clear window to look through.Because there are no blood vessels in the cornea, it is normally clear and has a shiny surface. The cornea is extremely sensitive – there are more nerve endings in the cornea than anywhere else in the body.
Iris
The colored part of the eye is called the iris.It controls light levels inside the eye similar to the aperture on a camera. The round opening in the center of the iris is called the pupil. The iris is embedded with tiny muscles that dilate (widen)and constrict (narrow) the pupil size. The sphincter muscle lies around the very edge of the pupil. In bright light, the sphincter contracts, causing the pupil to constrict. The dilator muscle runs radially through the iris, like spokes on a wheel. This muscle dilates the eye in dim lighting. The iris is flat and divides the front of the eye (anterior chamber) from the back of the eye (posterior chamber). Its colour comes from microscopic pigment cells called melanin. The colour,texture, and patterns of each person’s iris are as unique as a fingerprint.
Lens
The crystalline lens is located just behind the iris. Its purpose is to focus light onto the retina. The nucleus, the innermost part of the lens, is surrounded by softer material called the cortex. The lens is encased in a capsular-like bag and suspended within the eye by tiny “guy wires” called zonules. In young people, the lens changes shape to adjust for close or distance vision. This is called accommodation. With age, the lens gradually hardens, diminishing the ability to accommodate.
Retina
The retina is a multi-layered sensory tissue that lines the back of the eye. It contains millions of photoreceptors that capture light rays and convert them into electrical impulses. These impulses travel along the optic nerve to the brain where they are turned into images. There are two types of photoreceptors in the retina: rods and cones.
Rods and Cones
There are about 125 million rods and six to seven million cones in an average eye.
The cones are located in the central yellow part of the eye known as the macula. In the central part of the macula is the fovea centralis, a 0.3mm rod free area where cones are thin and densely packed. The cones are responsible for colour and high resolution vision. When viewing a scene, the eyes move continually to keep the light from the object of interest falling on the fovea where the bulk of the cones reside.
The rods are more than 1000 times as sensitive to light than the cones but are not sensitive to colour. It is thought that individual photons of light can trigger a rod under optimal conditions. Given the extra light sensitivity of rods it is possible for dimly lit objects like stars to be visible when seen in the peripheral vision but not to be visible when looked at directly. Rods are distributed away from the fovea and are therefore responsible for our perpherial vision.
The light response of the rods peaks sharply in the wavelengths associated with blue light and they respond very little to red light.
While the visual acuity or visual resolution is much better with the cones, the rods are better motion sensors.You can detect motion better with your peripheral vision, since it is primarily rod vision.
Optic Nerve
The optic nerve transmits electrical impulses from the retina to the brain. It connects to the back of the eye near the macula.
Visual Acuity
The capacity of the eye to resolve detail is termed ‘acuity’. Acuity is dependent on the sharpness of the retinal focus within the eye and the sensitivity of the interpretative faculty of the brain. Acuity is not evenly distributed across the retina, this is because the high resolution sensors (cones) are located predominately around the fovea. Everything that we see in detail is automatically bought into focus on the fovea. The rest of the retina which consists mostly of cones fills in the remainder of the picture in relatively coarse detail and brings to our attention any movement or change.
The quantitative measurement of visual acuity is a measure of the ability to distinguish black symbols against a white background. ’20/20 vision’ or its metric equivalent ‘6/6 vision’ is achieved where the person can distinguish objects which are seperated by 1 minute of arc. The numerator refers to the distance from which a person can reliably distinguish a pair of objects, the denominator is the distance from which an ‘average’ person would be able to distinguish objects with a seperation angle is 1 arc minute.
Visual acuity is measured using a Snellen Eye Chart.
Light Adaptation
There are basically two ways that the eye can adapt to changing levels of light. The first is by changing the diameter of the iris, this can change very rapidly and can alter the amount of light entering the eye by a ratio of 5 : 1. The second method of adapting for changing light levels is through chemical changes in the retina, these changes take place relatively slowly. It takes about seven minutes for full dark adaption of the cones and up to another 30 minutes for full rod adaption. Through this process however the eye can adapt to variations of light levels in the order of 150,000 : 1.
Eye Conditions
In this section we will look at eye conditions which are not disease related but instead occur as a result of differences in the shape or function of parts of the eye. There are numerous diseases of the eye which affect vision which are not covered in this section.
MyopiaMyopia or nearsightedness, occurs when light entering the eye focuses in front of the retina instead of directly on it. This is caused by a cornea that is steeper, or an eye that is longer, than a normal eye. Myopia is fairly common worldwide. Approximately 25% of the population is myopic to some degree, affecting men and women equally. There is greater prevalence of this disorder among children from higher socio-economic groups. Incidence is much higher in certain Asian countries with Taiwan experiencing the worlds highest rate. |
 |
HyperopiaHyperopia, or farsightedness, is a common vision problem, affecting about a fourth of the population. Farsightedness or hyperopia, occurs when light entering the eye focuses behind the retina, instead of directly on it. This is caused by a cornea that is flatter, or an eye that is shorter, than a normal eye. Farsighted people usually have trouble seeing up close, but may also have difficulty seeing far away as well. Young people with mild to moderate hyperopia are often able to see clearly because their natural lens can adjust, or accommodate to increase the eye’s focusing ability. However, as the eye gradually loses the ability to accommodate due to not using our eyes properly, not exercising them, blurred vision from hyperopia often becomes more apparent. The degree of your farsightedness determines your focusing ability. People who are severely farsighted are able to see clearly only objects that are a great distance away from their eyes. If you’re mildly farsighted, you may be able to see clearly objects that are closer to you. |
 |
AstigmatismAstigmatism is caused by any incorrect shaping of the cornea and results in the inability of the cornea to properly focus an image onto the retina. Usually the cornea is spherically shaped, like a baseball. However, in astigmatism the cornea is elliptically shaped, more like a football. A person with nearsightedness (myopia) or farsightedness (hyperopia) may see a dot as a blurred circle. A person with astigmatism may see the same dot as a blurred oval or frankfurter-shaped blur. |
  |
PresbyopiaPresbyopia is generally believed to stem from a gradual loss of flexibility in the natural lens inside your eye although changes in the lens’s curvature from continual growth and loss of power of the ciliary muscles (the muscles that bend and straighten the lens) have also been postulated as its cause. The eye’s lens stiffens with age, so it is less able to focus when you view something up close. The result is blurred near vision. Presbyopia is different from near-sightedness or Myopia because Myopia is caused by an abnormally shaped eye ball or cornea while Presbyopia relates to the lens. These age-related changes occur within the proteins in the lens, making the lens harder and less elastic with the years. Age-related changes also take place in the muscle fibres surrounding the lens. With less elasticity, the eye has a harder time focusing up close. Presbyopia is a refractive error, which results from a disorder rather than from disease. A refractive error means that the shape of your eye does not bend light correctly, resulting in a blurred image. |
 |
Limitations on Vision for Pilots
Night Vision
The rods are responsible for vision in low light levels (scotopic vision) and the cones function at higher light levels (photopic vision). Photopic vision provides a fine level of detail (20/20 – 6/6) and the capability to see colour. Scotopic vision provides only a coarse level of detail (20/200 – 6 / 60), can function at very low light levels but only provides the ability to distinguish between various shades of black and white. This limitation can be verified by looking at brightly coloured objects like flowers in fading light, the colours appear to wash out as the light fades.
The transition zone between photopic and scotopic vision where the level of illumination is equivalent to twilight or dusk, is called mesopic vision. Neither the rods nor the cones operate at peak efficiency in this range, but both actively contribute to visual perception. Mesopic vision may be of primary importance to the aviator at night because some light is often present during night operations. Below the intensity of moonlight, the cones cease to function and the rods alone are responsible for what is pure scotopic vision.
Dark adaptation is an independent process during which each eye adjusts from a high-luminance setting to a low-luminance setting. Both rods and cones contain light-sensitive chemicals called photopigments.Upon exposure to light, photopigments undergo a chemical reaction that converts light energy to electrical activity, initiating visual impulses in the retina that are conducted by nerve fibers from the eye to the brain. The initial chemical reaction is called light adaptation and, in this process, the photopigments are decomposed. Intense light will decompose the photoreceptor pigments rapidly and completely, thus reducing retinal sensitivity to dim light. Regeneration of the photopigments occurs during dark adaptation.
The fully dark-adapted eye, in which photopigment regeneration is complete, restores retinal sensitivity to its maximal level. Rods and cones differ markedly, however, in their rate of dark adaptation. Cones attain maximum sensitivity in 5-7 minutes, while rods require 30-45 minutes or longer of absolute darkness to attain maximum sensitivity after exposure to bright light.
The effect of hypoxia on night vision is primarily one of an elevation of the light levels required for detection by the rods and cones. Cone function loss has been clearly demonstrated by the loss of color vision at hypoxic altitudes, but the reduction of central visual acuity is usually insignificant. However, scotopic night vision at altitude can be significantly reduced. Scotopic vision has been reported to decrease by 5% at 3,500 feet, 20% at 10,000 feet, and 35% at 13,000 feet, if supplemental oxygen is not provided. Thus, the use of oxygen, even at low pressure altitudes, can be very important at night.
Physiologic Blind Spot
Each eye has a physiologic blind spot. Unlike the central blind spot that is only present in low light, the physiologic blind spot is always present. It is caused by the position of the optic nerve in the rear of the eye. The optic nerve is the confluence of retinal nerve fibers leaving the eye. There are no retinal receptors overlying the optic nerve. Fortunately, the physiologic blind spots occur in a different position in each eye. Thus, when both eyes are open, the physiologic blind spots are not apparent.
Empty Field Myopia
A pilot who experiences empty-field myopia is a pilot who is unable to see an aircraft or obstruction in the distance, despite the unrestricted visibility. To see something, the lens of the eye must be capable of physically focusing light from the object on the retina. To do this, the eye must be stimulated by an image. If the eye lacks this stimulation, the lens shifts to a resting state some one to two metres away.
When the sky is featureless—as is the case with unrestricted visibility, with hazy conditions, dark night conditions or in fog or cloud – you effectively become near-sighted when you look out as your eyes tend to resort to their natural resting state.
To counter empty-field myopia, it is a good practice to focus quite frequently on your own aircraft wing tips or in the case of a balloon, at the top of the balloon. Also, when scanning, focus on distant visible objects or outlines at or near the horizon, stimulating the eyes to establish long-distance focal points.
Technical data content credited to Mr Steve Griffin